![]()
Full CPHQ Practice Test and 635 unique questions with explanations waiting just for you!
CPHQ Certification Dumps CPHQ Exam for Full Questions - Exam Study Guide
NAHQ CPHQ exam is a comprehensive assessment that evaluates the ability of healthcare quality professionals to improve quality outcomes and patient safety. CPHQ exam covers a wide range of topics, including quality management, performance measurement, patient safety, and healthcare regulations. Candidates who pass the exam are considered experts in healthcare quality and are well-equipped to lead quality improvement initiatives.
The healthcare industry is constantly evolving and improving to meet the needs of patients worldwide. With this growth comes the need for professionals who are knowledgeable and skilled in ensuring quality patient care. This is where the NAHQ CPHQ (Certified Professional in Healthcare Quality) certification exam comes into play.
NAHQ CPHQ Certification Exam is a computer-based test that consists of 125 multiple-choice questions. CPHQ exam is administered at Pearson VUE testing centers located throughout the United States and internationally. Candidates have four hours to complete the exam.
NEW QUESTION # 233
The culture of safety survey data below is collected from perioperative services. Which action should the healthcare quality professional recommend?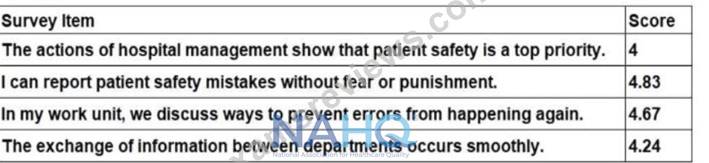
- A. Establish a process for executive walk-arounds in the perioperative departments.
- B. Implement a leadership training series on Just Culture principles.
- C. Develop a team-based communication training for perioperative staff.
- D. Educate perioperative staff on how to submit incident reports.
Answer: A
Explanation:
The culture of safety survey data provides insights into the perceptions of perioperative staff regarding patient safety practices, scored on a scale (typically 1 to 5, where 5 is the highest). The scores are as follows: hospital management's prioritization of safety (4), reporting mistakes without fear (4.83), discussing error prevention (4.67), and interdepartmental information exchange (4.24). The lowest score is 4 for the item "The actions of hospital management show that patient safety is a top priority," indicating a relative weakness in visible leadership commitment to safety, which is a critical component of a strong safety culture.
According to NAHQ CPHQ study materials, a key principle of a culture of safety is the visible commitment of leadership to patient safety, as it sets the tone for the organization and influences staff behavior. The score of 4 suggests that while staff perceive some prioritization, there is room for improvement in how management demonstrates this commitment. Establishing a process for executive walk-arounds in the perioperative departments (B) directly addresses this gap by increasing leadership visibility, fostering open communication, and demonstrating that patient safety is a priority. Walk-arounds allow leaders to engage with staff, observe processes, and address safety concerns in real-time, which can improve perceptions of leadership commitment.
Implementing a leadership training series on Just Culture principles (A) is relevant for the high score of 4.83 in reporting without fear, but this area is already strong, and the survey does not indicate a punitive culture needing immediate focus. Developing team-based communication training (C) could address the score of 4.24 for interdepartmental information exchange, but this is not the lowest-scoring item, and communication issues are secondary to leadership visibility in this context. Educating staff on incident reporting (D) is unnecessary given the high score of 4.83 for reporting without fear, indicating staff are already comfortable with reporting.
NAHQ emphasizes addressing the weakest areas of a safety culture first, making leadership visibility the priority here, thus option B is the recommended action.
Reference: NAHQ CPHQ Study Guide, Patient Safety Section, "Culture of Safety and Leadership Engagement"; NAHQ CPHQ Practice Exam, Safety Culture Assessment and Interventions.
NEW QUESTION # 234
A pulmonologist is gathering social determinants of health data from their patients. Which of the following best explains the purpose of collecting this data?
- A. This information facilitates the patient's application for state resources
- B. This information is needed to meet a new quality metric
- C. This evaluates connections between the disease and the living conditions
- D. This is a result of an update to the electronic medical record system
Answer: C
Explanation:
Social determinants of health (SDOH) are non-medical factors (e.g., housing, education, income) that influence health outcomes. Collecting SDOH data helps providers understand and address these factors to improve care.
Option A (This evaluates connections between the disease and the living conditions): This is the correct answer. NAHQ CPHQ study materials state that SDOH data is collected to identify how factors like housing instability or food insecurity impact diseases (e.g., asthma exacerbations in poor living conditions), enabling tailored interventions to improve outcomes.
Option B (This information is needed to meet a new quality metric): While SDOH data may contribute to quality metrics, the primary purpose is to understand health impacts, not just compliance with metrics.
Option C (This is a result of an update to the electronic medical record system): EMR updates may facilitate SDOH data collection, but they are a tool, not the purpose of the data collection.
Option D (This information facilitates the patient's application for state resources): SDOH data may support resource referrals, but the primary goal is to evaluate health impacts, not solely to secure resources.
Reference: NAHQ CPHQ Study Guide, Domain 5: Population Health and Care Transitions, emphasizes SDOH data collection to evaluate connections between living conditions and health outcomes.
NEW QUESTION # 235
Members of a performance improvement team voice complaints about not having as much decision-making authority as they expected. Which of the following should be developed to decrease the likelihood of such complaints?
- A. team charter
- B. interrelationship diagram
- C. project checklist
- D. affinity diagram
Answer: A
Explanation:
A team charter is a document that outlines the purpose, scope, and objectives of the team, including roles, responsibilities, and decision-making authority. Developing a team charter helps prevent complaints about lack of decision-making authority by:
* Clarifying Roles and Responsibilities:
* The team charter explicitly defines each member's role, their level of decision-making authority, and the boundaries within which they operate. This helps to set clear expectations from the outset.
* Establishing Clear Guidelines:
* The charter provides a framework for how decisions are made, who needs to be consulted, and the process for escalating issues. This minimizes confusion and ensures that all team members are aware of their responsibilities and limitations.
* Preventing Miscommunication:
* By outlining the decision-making process and authority levels in the charter, it reduces the risk of miscommunication and misunderstanding about what the team can and cannot decide.
* Building Consensus:
* The development of the charter often involves the team itself, which can help build consensus and buy-in, ensuring that all members agree on the scope of their authority.
Other options like a project checklist, affinity diagram, or interrelationship diagram, while useful in different contexts, do not address the specific need for clarifying decision-making authority.
References:
* NAHQ Guide to Team Management and Leadership in Healthcare
* NAHQ Resources on Effective Team Development
=========
NEW QUESTION # 236
Which initiative should a quality professional promote in an organization seeking to optimize value-based reimbursement?
- A. Standardize joint replacement care pathways.
- B. Reduce use of inpatient restraints.
- C. Improve hand hygiene compliance.
- D. Implement computerized provider order entry (CPOE).
Answer: A
Explanation:
In an organization seeking to optimize value-based reimbursement, a healthcare quality professional should promote initiatives that directly impact clinical outcomes, patient satisfaction, and cost-efficiency.
Standardizing joint replacement care pathways (Answer A) is an initiative that aligns with these goals. By ensuring consistency in care, reducing variability, and following evidence-based practices, standardized pathways improve outcomes, decrease complications, and reduce costs, which are all critical components in value-based reimbursement models.
The other initiatives, while beneficial, are not as directly linked to optimizing value-based reimbursement:
* Improving hand hygiene compliance (B) is essential for infection control but has a more indirect impact on value-based reimbursement.
* Reducing the use of inpatient restraints (C) focuses on patient safety and ethical care, which is important but not directly related to reimbursement optimization.
* Implementing computerized provider order entry (CPOE) (D) can reduce errors and improve efficiency, but its impact on value-based reimbursement is broader and less direct compared to standardized care pathways.
References:
* National Association for Healthcare Quality (NAHQ) - Certified Professional in Healthcare Quality (CPHQ) Study Materials.
* Value-Based Reimbursement Strategies, NAHQ Documentation.
* Clinical Pathway Standardization and Its Impact on Value-Based Care, NAHQ Resources.
=========
NEW QUESTION # 237
Quality and technical performance refers to how well current scientific medical knowledge and technology are applied in a given situation.
It is usually assessed in terms of:
- A. Both A and B
- B. Timeliness and accuracy of the diagnosis
- C. Appropriateness of therapy and other medical interventions are performed
- D. The quality of interpersonal relationships
Answer: A
NEW QUESTION # 238
A pay-for-performance structure includes a payout based on achieving the NCQA Quality Compass 50th Percentile, plus an additional bonus for achieving the NCQA Quality Compass 75th Percentile. Individual performance on measures is as follows:
NCQA Measure
Physician A
Physician B
Nurse Practitioner C
Physician Assistant D
50th Percentile
75th Percentile
Diabetic Retinal Eye Exam
75%
80%
60%
63%
65%
70%
Nephropathy
53%
43%
50%
48%
50%
52%
HbA1c Testing
76%
80%
52%
70%
72%
76%
Which provider will not earn pay-for-performance based on reaching either the NCQA Quality Compass
50th or 75th percentile?
- A. Nurse Practitioner C
- B. Physician A
- C. Physician Assistant D
- D. Physician B
Answer: A
Explanation:
To determine which provider does not earn pay-for-performance, we must compare each provider's performance against the 50th and 75th percentiles for all measures. A provider must meet at least the 50th percentile on at least one measure to qualify.
Physician A: Diabetic Retinal Eye Exam (75% > 65% [50th], > 70% [75th]), Nephropathy (53% > 50%
[50th], > 52% [75th]), HbA1c Testing (76% = 76% [75th], > 72% [50th]). Meets 50th and 75th percentiles on multiple measures, qualifying for payout.
Physician B: Diabetic Retinal Eye Exam (80% > 65% [50th], > 70% [75th]), Nephropathy (43% < 50%
[50th]), HbA1c Testing (80% > 72% [50th], > 76% [75th]). Meets 50th and 75th percentiles on two measures, qualifying for payout.
Nurse Practitioner C: Diabetic Retinal Eye Exam (60% < 65% [50th]), Nephropathy (50% = 50% [50th], <
52% [75th]), HbA1c Testing (52% < 72% [50th]). Meets only the 50th percentile for Nephropathy, but performance is below 50th for other measures, and no 75th percentile is met, making this the weakest performer.
Physician Assistant D: Diabetic Retinal Eye Exam (63% < 65% [50th]), Nephropathy (48% < 50% [50th]), HbA1c Testing (70% < 72% [50th]). Does not meet 50th percentile on any measure, potentially disqualifying them.
Analysis: The question asks for the provider who does not earn pay-for-performance based on reaching either percentile. Nurse Practitioner C meets the 50th percentile for Nephropathy (50%), while Physician Assistant D meets no percentiles. However, the phrasing suggests a single provider, and C's minimal achievement (only one measure at 50th) may be interpreted as insufficient for payout, depending on program rules. Given C's overall poor performance (below 50th on two measures), it is the most likely answer.
CPHQ Objective Reference: Domain 2: Health Data Analytics, Objective 2.4, "Interpret performance data for pay-for-performance programs," requires comparing provider data against benchmarks. The NAHQ study guide notes, "Providers must meet or exceed percentile thresholds to qualify for pay-for-performance incentives" (Domain 2).
Rationale: Nurse Practitioner C's marginal performance (only one measure at 50th, none at 75th) makes them the least likely to earn payout, aligning with CPHQ's focus on data-driven performance evaluation.
Reference: NAHQ CPHQ Study Guide, Domain 2: Health Data Analytics, Objective 2.4.
NEW QUESTION # 239
The quality of amenities of care refers to the characteristics of the setting in which the encounter between patient and clinician takes place, such as:
- A. Responsive to patient preferences
- B. Comfort, convenience and privacy
- C. Comfort
- D. Comfort, care and access
Answer: B
NEW QUESTION # 240
What is the initial step an organization should take when the strategic goal of improving patient satisfaction has not been met?
- A. Implement benchmarking
- B. Conduct a root cause analysis
- C. Review department-specific data
- D. Perform a needs assessment
Answer: B
Explanation:
Failing to meet a strategic goal like improving patient satisfaction requires identifying the underlying reasons for the shortfall to inform effective interventions.
Option A (Implement benchmarking): Benchmarking compares performance to peers, useful later but not the initial step to understand internal issues.
Option B (Review department-specific data): Data review is part of root cause analysis but is too narrow as an initial step, as it assumes departmental issues.
Option C (Perform a needs assessment): Needs assessments identify gaps in resources or training, but they follow understanding the cause of failure.
Option D (Conduct a root cause analysis): This is the correct answer. The NAHQ CPHQ study guide states,
"When a strategic goal like patient satisfaction is not met, the initial step is to conduct a root cause analysis to identify underlying causes, such as process or communication failures" (Domain 4). RCA uses tools like fishbone diagrams to pinpoint issues.
CPHQ Objective Reference: Domain 4: Performance and Process Improvement, Objective 4.5, "Identify causes of performance gaps," emphasizes RCA for unmet goals. The NAHQ study guide notes, "RCA is critical to understand why strategic objectives are not achieved" (Domain 4).
Rationale: RCA identifies the root causes of the satisfaction gap, aligning with CPHQ's improvement principles.
Reference: NAHQ CPHQ Study Guide, Domain 4: Performance and Process Improvement, Objective 4.5.
NEW QUESTION # 241
In reviewing information offered by the Agency for Healthcare Research and Quality (AHRQ), the quality improvement (QI) specialist recognizes that the three broad aims pursued by the National Quality Strategy are
- A. reduce medical waste, use Lean, and achieve equity and better access to care.
- B. better care, healthy people/health communities, and affordable care.
- C. triple aim, reduce utilization, and affordable care.
- D. reduce complications, reduce readmissions, and improve health outcomes.
Answer: B
Explanation:
The three broad aims pursued by the National Quality Strategy (NQS), as recognized by the Agency for Healthcare Research and Quality (AHRQ), are better care, healthy people/healthy communities, and affordable care. These aims reflect a comprehensive approach to improving healthcare by focusing on enhancing the overall quality of care, improving the health of populations, and reducing the cost of care to ensure it is affordable for all.
* Reduce medical waste, use Lean, and achieve equity and better access to care (A): These are important goals, but they do not summarize the NQS's broad aims.
* Reduce complications, reduce readmissions, and improve health outcomes (B): These are specific targets within the broader framework but not the three broad aims.
* Triple aim, reduce utilization, and affordable care (D): The triple aim concept is related, but it is not identical to the three broad aims of the NQS.
References
* NAHQ Body of Knowledge: National Quality Strategy and Healthcare Improvement
* NAHQ CPHQ Exam Preparation Materials: Understanding National Quality Initiatives
=========
NEW QUESTION # 242
A healthcare organization has two years of data on infection rates by month. Which of the following process tools would be best to use for analyzing this data?
- A. Run chart
- B. Fishbone diagram
- C. Pareto chart
- D. Histogram
Answer: A
Explanation:
A run chart is a line graph that displays data points over time, making it ideal for analyzing trends in infection rates on a monthly basis. It helps in identifying patterns, shifts, or cycles in the process, which is essential for monitoring and improving infection control practices.
References:
NAHQ CPHQ Exam Preparation Materials: Health Data Analytics
NAHQ Body of Knowledge: Health Data Analytics
NEW QUESTION # 243
Which of the following is the most effective means of communicating commitment to patient safety?
- A. articles by a CEO in the employee newsletter
- B. posters and bulletin boards on units displaying up-to-date patient falls data
- C. senior leaders having discussions on units with front-line staff
- D. CEO presenting most recent medication error rates to the governing body
Answer: C
Explanation:
Effective communication in healthcare is paramount for patient safety. It is the accurate transfer of information between two or more providers1. Communication fails when it is incomplete, ineffective, or inappropriate, resulting in patient harm1. Good teamwork and effective communication rely on mutual respect, problem-solving, and sharing of ideas1.
Senior leaders having discussions on units with front-line staff is a direct and effective means of communication. It allows for immediate feedback, clarification of doubts, and a better understanding of the situation on the ground2. This direct interaction can foster a culture of safety, encourage the sharing of ideas, and promote problem-solving1.
In contrast, the other options (A, B, and C) are less direct and may not effectively communicate the commitment to patient safety. For example, presenting error rates or displaying data on bulletin boards (options A and C) are important but may not lead to immediate action or feedback. Similarly, articles in a newsletter (option B) may not reach all staff or may not be read thoroughly.
Reference: 1, 2
https://psnet.ahrq.gov/perspective/approach-improving-patient-safety-communication
NEW QUESTION # 244
The percentage of patients with congestive heart failure who are receiving an ACE inhibitor is an example of
retrospective measure. The use of ACE inhibitors in the population is indicated for all patients with an ejection
fraction of less than 40 percent. The ejection fraction is not part of the typical administrative database. Sometimes the
information is contained:
- A. In a separate computer record
- B. In an ERP system
- C. In a stand-alone database in cardiology department and is generated in accessible
- D. In a worksheet
Answer: C
NEW QUESTION # 245
A director at a large health system is tasked with building a new population health program.
What is the director's first step?
- A. Implement artificial intelligence programs to stratify patients into categories of risk.
- B. Analyze the data infrastructure capabilities and sources of information.
- C. Identify strategies to incorporate social determinants of health screenings.
- D. Design a complex care management program focused on chronic health conditions.
Answer: B
Explanation:
The first step in building a new population health program is to analyze the data infrastructure capabilities and sources of information. Effective population health management requires robust data collection, integration, and analysis capabilities to identify and stratify patient populations, track health outcomes, and monitor program effectiveness. Understanding the current data infrastructure will enable the director to assess whether the existing systems can support the new program and what enhancements may be needed.
Implement artificial intelligence programs to stratify patients into categories of risk (A): While important, this is a later step that depends on having a solid data infrastructure in place.
Identify strategies to incorporate social determinants of health screenings (B): This is also crucial but should follow an understanding of the data infrastructure and capabilities.
Design a complex care management program focused on chronic health conditions (C): Designing the program is important but must be informed by a thorough analysis of the data capabilities.
Reference
NAHQ Body of Knowledge: Data Management in Population Health Programs
NAHQ CPHQ Exam Preparation Materials: Steps to Building a Population Health Program
NEW QUESTION # 246
Which of the following would be the best methodology to reduce referral wait time?
- A. Six Sigma
- B. Plan-Do-Study-Act
- C. Rapid cycle improvement
- D. Lean
Answer: D
Explanation:
Detailed Explanation:
Lean methodology focuses on identifying and eliminating waste in processes, such as delays in referral wait times. It streamlines workflows to increase efficiency and reduce wait times.
Option A: Lean
Lean is specifically designed to eliminate inefficiencies and streamline processes, making it ideal for reducing wait times.
Other Options:
Six Sigma focuses on reducing defects rather than waste.
Rapid cycle improvement and PDSA are effective for testing small changes but may not directly target waste reduction in the same way as Lean.
References:
Lean methodology, as covered in CPHQ resources, is effective for reducing inefficiencies and delays, especially in healthcare referral processes.
NEW QUESTION # 247
A healthcare quality professional is charged with facilitating a team. The goal of the team is to develop criteria for levels of care in behavioral/mental health. Which of the following is the most important characteristic of the facilitator?
- A. ability to moderate a work group
- B. knowledge of levels of care
- C. knowledge of behavioral/mental health
- D. ability to select team members
Answer: A
Explanation:
The ability to moderate a work group (C) is the most important facilitator characteristic, ensuring effective collaboration and progress. Selecting members (A) and knowledge of mental health (B) or levels of care (D) are secondary. NAHQ prioritizes moderation skills.
NAHQ CPHQ Study Guide, Performance and Process Improvement Section, "Team Facilitation Skills"; NAHQ CPHQ Practice Questions, Quality Team Dynamics.
NEW QUESTION # 248
Which of the following is a key component in establishing a comprehensive population health management program?
- A. Data infrastructure
- B. A business plan demonstrating expected cost savings
- C. Partnership with an accountable care organization
- D. Patient satisfaction metrics
Answer: A
Explanation:
Population health management (PHM) aims to improve the health outcomes of a group by monitoring and identifying individual patients within that group. A robust data infrastructure is fundamental to the success of PHM programs. It enables the collection, analysis, and sharing of health data across various platforms and stakeholders, facilitating informed decision-making and effective management of patient populations.
A comprehensive data infrastructure supports:
* Information-Powered Clinical Decision-Making: By integrating and analyzing data from diverse sources, healthcare providers can make evidence-based decisions tailored to individual patient needs.
* Identification of High-Risk Patients: Advanced data analytics can stratify patient populations to identify individuals at higher risk, allowing for targeted interventions.
* Performance Monitoring: Continuous data collection and analysis enable healthcare organizations to monitor outcomes, assess the effectiveness of interventions, and make necessary adjustments to improve care quality.
While partnerships with accountable care organizations (Option A), business plans demonstrating cost savings (Option B), and patient satisfaction metrics (Option D) are important elements in healthcare management, they are not as foundational as a robust data infrastructure in establishing a comprehensive PHM program.
References:
* American Hospital Association - "Three Key Elements for Successful Population Health Management" aha.org
* Southern New Hampshire University - "What is Population Health Management?" snhu.edu
NEW QUESTION # 249
Which of the following strategies promotes timely completion of a quality improvement project?
- A. assigning the team leader to document overall project progress
- B. focusing routine senior leader updates on project successes
- C. requiring team members to devote a majority of their time to project work
- D. allowing the project sponsor to direct the project team's work
Answer: A
Explanation:
Assigning the team leader to document overall project progress is a strategy that promotes timely completion of a quality improvement project. The team leader is responsible for overseeing the project, tracking progress, and ensuring that milestones are met. By documenting progress, the team leader can identify potential delays or issues early, coordinate efforts to address them, and keep the project on schedule.
* Allowing the project sponsor to direct the project team's work (A): The sponsor provides support and resources but should not be involved in day-to-day project management.
* Requiring team members to devote a majority of their time to project work (C): While important, this may not be feasible and does not ensure timely completion if not managed properly.
* Focusing routine senior leader updates on project successes (D): While recognizing successes is important, it should not be the sole focus, as it might overlook areas needing attention.
References
* NAHQ Body of Knowledge: Project Management and Leadership in Quality Improvement
* NAHQ CPHQ Exam Preparation Materials: Strategies for Timely Project Completion
=========
NEW QUESTION # 250
......
Authentic Best resources for CPHQ Online Practice Exam: https://easypass.examsreviews.com/CPHQ-pass4sure-exam-review.html